

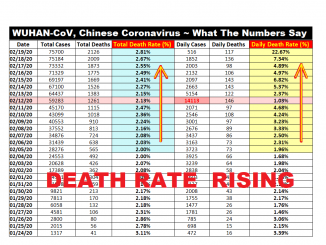
Part 2 in Series has now been released, and discusses Wuhan-CoV Death Rates, and how they are being misreported.
PERSONAL BACKGROUND: I was one of the 1st people back in the early 2000’s covering the original SARS Outbreak. I researched and followed SARS, then H5N1, H1N1, MERS, and more recently the H7n9 viruses. I recently started watching this Chinese 2019-NCoV Virus a month ago. Based on years of research, I have become concerned that important information is NOT being publicly communicated. This article attempts to provide some perspective on certain aspects of the developing situation that I feel are not being properly addressed.
SITUATIONAL BACKGROUND: Coronaviruses are in a family of viruses that most people associate with the common cold. They are much smaller in size than Influenza viruses, which is a primary factor for why they spread so easily. They also can live outside a host longer (e.g. on doorknobs, tabletops, in the air, etc.) Historically Coronaviruses were simply an annoying part of life (stuffy noses and sneezes) – until 2003 with the mutation of SARS out of China, and then around 2015 with the Saudia Arabian MERS mutation. These viruses “mutate” (change over time) easily, but they are more stable than Influenza viruses, which change very rapidly. The changes that occurred with SARS and MERS were not “good” changes. SARS killed an estimated 9.5% of people infected. Global infections reached 8,098 people of which 774 died. Some health experts believe many deaths were mistakenly attributed to Influenza at the time, and the total SARS mortality could have been as high as 15%. MERS is estimated to have a 30% – 40% mortality (death) rate. In both SARS and MERS there have been smaller clusters with substantially higher mortality rates.
The newest 2019-NCoV began in early December 2019, and stands for a 2019 Virus that is a Novel (new) Coronavirus. For simplicity sake, I will now name the virus “WUHAN-CoV” and all such references hereafter shall relate to the 2019-NCov virus that is now spreading. WUHAN-CoV has been genetically identified to have originally mutated into the human species via a zoonotic (animal>human) shift from Bats, similar to SARS.
WUHAN-CoV INFECTION, SPREAD, MISC FACTS:
These are the first important bits of information that the public needs to know.
1) SIZE IMPACTS SPREAD VIA AIRWAY TRANSMISSION: As mentioned earlier, Coronaviruses are very small. There are variations, but for simplicity sake I am going to take some averages when discussing size. Influenza viruses are about 0.3 microns in diameter. An N95 Mask blocks 95% of all particles that are 0.3 microns in diameter or larger. Coronaviruses are much smaller at a range of 0.06 – 0.14 microns. A standard N95 mask is going to be virtually useless in stopping the spread of the virus, as it will pass through the larger openings in an N95 mask at above the effective protection rate. It is simply an issue of particle size, and the physics of a very small virus going through a larger opening. The cheaper masks that most people use are even less effective in preventing a person from catching WUHAN-CoV in a situation in which someone has sneezed, and the virus is floating around in the air, and you walk through that cloud of aerosolized virus mist. It gets worse. Because it is smaller in size, WUHAN-CoV will “float” in aerosolized form longer than a traditional Influenza Virus. Once it does settle somewhere, a countertop that you might lean on for example, it will also survive longer on that surface also, just waiting to transfer onto your hands, and for you to then touch your eyes, mouth, or nose (or open sore/cut). HOWEVER: the use of masks in high risk places will still be valuable, as they will catch some of the virus, and could reduce the “Viral Load” of exposure. Also – the use of masks by people that are sick is absolutely mandatory to help reduce the spread. The inside of the masks greatly helps trap the viruses as they are suddenly expelled via cough, breath or sneeze. In short it dramatically cuts down on the amount of airborne virus release. If you are taking care of a sick family member at home – it is possibly more important that the sick person wear a mask than the caregiver – although both are recommended.
2) HEALTHCARE WORKER INFECTION: I am going to be blunt here, and tell you that the reason you are seeing so much concern in the Global Health Community is that WUHAN-CoV kills Healthcare Workers. Hanoi & Hong Kong Hospitals were hit hard in the 2003 SARS Outbreak, and many of the staff fled in some cases, fearing for their lives. Another example of this can be found in an Infamous Outbreak that occurred in a Toronto Canada Hospital (2nd very good study on larger Toronto Community Outbreak here). 144 Individuals were infected in the Toronto Hospital study. Of those, 111 people actually caught the infection in the hospital. Of those 73 were healthcare workers in the hospital. They eventually had to quarantine entire hospital medical staff – as they could not risk letting the virus escape back into the public. The approach worked, and the SARS Outbreak was stopped. Yet in this single local outbreak, 14% of the patients ended up requiring mechanical ventilation, and 5.6% ended up dying. Already in China, healthcare officials are building a new emergency hospital to ONLY take care of WUHAN-CoV cases – which is a lesson learned from the 2003 SARS Outbreak – that these patients need isolated treatment and cannot be mixed into normal Hospital procedure. Also in China, other hospitals have started erecting tents in parking lots specifically for WUHAN-CoV patients only. The important takeaway is that mixing this easily contagious virus into a closed air hospital system does nothing but cause exceptional risk to other patients, and medical personnel. And again – the simple explanation that they are not providing is very easy to understand: this is a tiny virus capable of getting through traditional protection (e.g. N95 masks), and because it is so easily aerosolized it can spread through ventilation systems – passing easily through traditional air filters designed to catch larger particles. All 3 of the reference story links above are good examples of what we could soon be facing on a global scale.
3) RISK OF SPREAD VIA CENTRAL AIRDUCTS: An example of this can be found in a study of the infamous SARS outbreak that involved the Amoy Gardens Housing Complex in China. At the end, 329 people in the highrise were infected, and 42 died (12.7%). The Study link above details how the virus spread through the centralized air ducts – similar to what one finds in most hospitals, modern highrises, schools, office buildings, and nursing homes. And again, because of the small size of the particles, traditional air filters do not stop the spread. Even within an individual home where one person becomes ill – the virus can spread through the central air system. I cannot stress enough how important this aspect is — that hospitals, retirement homes, people living in centrally connected housing complexes, and people treating sick family in private residences are going to be at higher risk if centralized airducts exist, potentially extreme risk in the some situations.
The above section may be the most important takeaway fact in this entire article for individuals and institutional housing managers – the need to upgrade filtration, possibly adding UV disinfection capability, or for people treating sick people at home to seal off vents, and rely on open windows.
4) AGE RELATED RISK: I did a case study of some groups of people that died in this outbreak in China. The first 8 deaths in Hubei Province for example were ages: 70, 53, 86, 65, 84, 81, 80, 82. One longer list showed that 72% of persons who died were over 65. Also high in the percentages were people with basically any sort of pre-existing conditions (e.g. high blood pressure, diabetes, heart issues, weakened immune, etc). This disease is going to have an extremely high mortality impact on the older population (55+).
5) MORTALITY RATE ESTIMATIONS: I am going to try and explain this with an actual example case study already referenced above in the Toronto Hospital Case Study. As previously mentioned, 144 people were infected, and out of these 5.6% died. But equally, and maybe more important – 20% were placed in Intensive Care, and 14% had to receive Mechanical Ventilation assistance. While most of these people lived, it also resulted in a hospital care environment that devolved into utter chaos – similar to what is already being seen in Wuhan China Hospitals. These people lived primarily because they DID receive ICU treatment and mechanical ventilation assistance – but fast forward into a future world in which heathcare is overburdened, can’t keep up with the patients, have run out of space, and mechanical ventilation equipment is limited – and you begin to severely increase the mortality rate. The percentage of people needing ICU and mechanical ventilation to live will increase – but the infrastructure to provide it won’t be there. They will most likely be turned away and told to self treat at home, which we are already seeing in MANY cases in China.
5) DETECTION COMPLICATIONS: Most Countries have begun screening airline passengers for fever / high temperature. The problem with that is that several people infected – even all the way to death – are NOT exhibiting fevers, and that throws a monkey wrench into health official and governmental claims that they are going to be able to contain the spread. Honestly, that horse left the barn weeks ago. This thing is going to spread worldwide, and is already well beyond any hope of containment.
6) FIRST SYMPTOMS: While Fever and Cough and Respiratory Symptoms are most often initially present, this is not always the case. Here is a quote from a medical professional in China. “In many clinical cases, the patients did not have typical respiratory symptoms such as fever and cough at the time of consultation, and only the first symptoms of digestive system symptoms: Such as mild appetite, fatigue, poor mentality, nausea, vomiting, diarrhea, etc .; first manifestations of neurological symptoms such as headache; first manifestations of cardiovascular system symptoms such as palpitation, chest tightness, etc .; first manifestations of ophthalmic symptoms such as conjunctivitis ; Only mild sore limbs or lower back muscles.” The important takeaway here is that this is not always a simple and clear diagnosis. People may have to make best guess judgement calls based upon their recent exposure risks.
7) INFECTION TIMES: This is another big one that is complicating detection and spread control, and has a certain social-psychological fear component. I will refer to the time the virus can survive on surfaces outside the body as the “environmental period”, which in this case is from hours to months, depending upon the surface (i.e. hard metal, shorter – vs – carpet, longer). One study showed that the half-life of another human coronavirus in the air was 67 hours, indicating that HALF of the virus died within that time – so a good assumption is that it can last in the air for several days and remain infectious. So Coronavirus has a very long environmental period. The “incubation period” is the time from which a person is exposed to the time that they show symptoms. So far that is looking like anywhere from 3 days to 14 days. The norm is loosely appearing to be 4 – 6 days. The “infection period” is the time in which an infected person can infect others. Studies and data have shown that a person can infect others well before symptoms have appeared, AND even after symptoms have disappeared and they appear cured. The biggest takeaway here is for people to realize that making decisions on whether to visit someone, to allow them to visit, or to attend a function based on whether people are showing obvious signs of sickness – is a Bad way to approach this. IF this becomes widespread in your community – the safest thing to do would be shelter in place and cut off contact. On a related note – while Coronaviruses do survive and spread in warmer seasonal weather, the high risk times are late fall, winter, and spring, similar to how the risk of Influenza goes down as the season warms. On a depressing note…. it is probable that this will be here for many seasons to come, and become as prevalent as the seasonal flu. As annual changes occur, so will severity levels.
8) INFECTION THROUGH EYES: There is already one report of a Chinese doctor infected simply because he slipped up for a brief time and took off his protective goggles. Shortly thereafter he noticed he had developed Conjunctivitis in a lower eyelid (red, puffy). The virus incubated in the eye fluids and then spread to the rest of his body. Goggles or eye-cover in a high risk setting that one might be exposed to aerosolized virus is highly recommended as well as some form of mask (which again is of limited protection – but does offer some protection).
9) PH-DEPENDENT: Coronaviruses are PH-Dependent, which means in this case that they reproduce and thrive more effectively in a low PH (acidic) environment. A High PH Environment (alkaline) is not favorable to their survival. One study has shown that some Coronaviruses at 37 degrees Celsius (Human Body Temp of 98.6 F) combined with a PH level of 8.0 kills the virus. A Neutral PH level is 7. Anything lower is Acidic. Higher is Alkaline. In regards to Coronaviruses – a higher Alkaline level is better for the person, and worse for the virus. Human blood PH levels are tightly controlled in an optimal 7.35 – 7.45 PH range. Intercellular Fluids however are not as tightly controlled and can range from a PH of 6.0 – 7.2 and can be moved more easily. The Intercellular fluids is where the Viruses reproduce, so this is the one that matters. Our modern diet (sugar, high carbs, etc) have tended towards more acidic levels. Changing your diet to foods and drinks that promote a higher PH will help. But understand that changing your overall body PH is a long, slow process that must be worked at – however the following items can move it quicker, especially at the intercellular fluid level. High PH (alkaline) Water supplements & Bicarbonate of Soda (Baking Soda) can increase PH levels. (Ref 1) (Ref 2) (Ref 3) (Ref 4) (and many others). For the record, you will never get your PH levels to 8.0 (and to do so would be UNhealthy) – but higher PH in general, even if slightly, creates a healthier body to fight off a Coronavirus or an Influenza infection. Considering that WUHAN-CoV is such a serious, high mortality strain, everything you do to give you an advantage, could mean the difference between life and death. Again, NOT a cure, but if you can get your Intercellular fluid PH levels to the high end of the range, then this will help. NOTE: There is a historical series of accounts that supports Baking Soda achieving success in this fight. During the 1918 Influneza Outbreak (Influenza is also PH Dependent) some accounts showed that drinking bicarbonate of soda mixtures showed dramatic increases in resistance & recovery, and now we know that there is some science behind it. This link has some mixture instructions from the early 19th Century that was claimed to work, and seems quite reasonable. Do NOT overdo it, nor is this a long term treatment, and make sure you have an aluminum free brand. Again, NOT a cure.
10) PROBIOTIC HEALTH: I am not going to go into great detail because this is already getting longer than most people want to read – but maintaining a very healthy probiotic environment in your gut and digestive tract has been used effectively as a strong component in treatment. Suffice it to say that building up your gut probiotics through yogurt, kefir, apple cider vinegar (a pre-biotic) and supplements is one of the top methods of lessening severity. Again, NOT a cure.
11) VACCINES AND MEDICATION TO THE RESCUE – NOT HAPPENING! : There is NO Vaccine, and none expected at any time in the near future. They have been trying to find one for the common cold (Coronavirus) for over a hundred years. Since the incredible scare of SARS in 2003 they put vaccine development on a fast track. MERS in 2015 increased the efforts. No luck. Nada. Zilch. Ain’t happening. I am not saying that it will never happen, but there is really nothing promising at present, and once they do get something, it will take a year+/- to realistically get it from concept to production. Health Officials or Media that throw this out as some form of “Hope” at the present time are being irresponsible.
SOME RANDOM TREATMENT THOUGHTS / FACTS:
Probiotics and PH balancing I’ve mentioned. There are other good, scientifically documented beneficial herbs and supplements that DO NOT CURE but can help to improve general health and increase immune response. I’m just going to randomly throw some things out for people to consider looking into.
12) PNEUMONIA: The primary disease mechanism in WUHAN-CoV that is of concern is the rapid development into Pneumonia. Whatever will aid in healing or treating pneumonia should be of value, so focus on pneumonia treatment if you want to do research. Decreasing Inflammation, and Increasing Oxygenation are the primary goals. Heat and Humidity are important – so a vaporizer and heating pad for use if sick would be something I would have on hand. Anything to open airways helps. Warm lemon water with honey is probably the most well known “folk remedy for a cold, as well as chicken soup (Ref 1; Ref 2). There actually IS science behind that – but make no mistake, these are NOT cures. THERE IS NO 100% CURE for this – the Goal here is in risk reduction to increase odds of survival, lessen infection time, reduce spread, etc. Pneumonia has specific symptoms but many causes, so I would study it if you want to know more. One thing to note is that this is NOT a common pneumonia, but is Coronavirus specific, so rumours that a Pneumonia Shot will prevent this are incorrect, although they could have secondary infection protection.
13) ORGAN FAILURE and SEPSIS (blood poisoning) is common in advanced cases. Good probiotic health aids in fighting secondary infections. Any sort of natural antioxidant, antibiotic, antiviral, or anti-inflammatory could also help. Examples could include: garlic (See Garlic Ref 1 / Ref 2 / Ref 3 / Ref 4 / Ref 5 / Ref 6 / Ref 7 / Ref 8 / Ref 9 ), ginger (See Ginger Ref 1; Ref 2), thyme, oregano oil, licorice (aka glycyrrhizin; See Ref 1 / Ref 2 / Ref 3 ), elderberry, reseveratol, curcumin/tumeric, Vitamin C, Vitamin D, and notably a new addition Zinc & Quercetin taken together are all high on the list. Thyme tea (fresh thyme + boiling water, without additives and well strained) makes an excellent eye rinse if you think you may have an infection vector in the eye (e.g. development of conjunctivitis after a recent potential exposure). There are anectotal stories, and some medical studies that indicate lemon juice can have a cleansing effect on the lungs. Keeping down secondary infections is incredibly important. As your body weakens, other bacteria and viruses can also take hold in what is known as Co-Infection. When your body gets over-run with bacteria it can start leaching into your blood system, and this leads to sepsis, which can lead to organ failures. Too much viral or bacterial infection leads to hyper Cytokine and Antibody activity, and this can lead to inflammation / rupture of cells which leads also to organ failure. At the first sign of possible infection, it is time to get ahead of things, and begin with antivirals and antibiotic assisting supplements (or medications if prescribed – just because I list a lot of herbs doesn’t mean you shouldn’t take advantage of medical treatment IF available). Remember that antibiotics can also kill the “good” probiotics also – so go heavy on probiotic supplementation during usage of antibiotics, whether medical or herbal or supplemental. NOT Cures.
IMPORTANT UPDATE JAN 25: An early paper just came out detailing initial WUHAN-CoV cases, which showed a 15% Mortality Rate in the 41 cases studied (see Table 3). I noticed 2 important takeaways that I have been concerned with and researching myself. #1) WUHAN-CoV is exhibiting signs of Cytokine Storm, similar to MERS & SARS, albeit at slightly lesser degree. Suffice it to say that this is BAD, and there is a reason I list this update under “Organ Failure & Sepsis” Section. “Cytokine Storm” is a phrase you see more and more often in both these Novel Coronaviruses and the newer, deadly influenzas such as H5N1, H7N9 etc. “Resveratol“ has shown potential against elevated Cytokine response (Ref 1) (Ref 2) (Ref 3) (Ref 4) (Ref 5) (Ref 6) (and many others), and anti-inflammatories like Tumeric/Curcumin are worth looking into. Ginger has show ability to reduce inflammation through Cytokine inhibition. Anti-histimines might show some promise. Garlic studies have shown that it has anti-infammatory and cytokine regulating ability. The earlier stage you get these going, the more benefit. Cytokine Storm causes massive and sudden inflammation that can cause organs to fail in later stages. #2) There has been long debate over whether or not giving Corticosteroids (i.e. Prednisone) is helpful in SARS, MERS, and now WUHAN CoV’s, or can actually worsen patient condition. This report contains more data that further weights towards “harm” not healing. NOT Conclusive. However, since Prednisone is such a go-to (often without even thinking) standard for most doctors, there needs to be an increased effort to educate medical professionals of the research data, and this is NOT happening in a satisfactory manner.
Again, NOTHING mentioned here is a Cure.
14) VIRAL LOAD: ***VERY IMPORTANT***: Viral load represents the amount of virus you are fighting. Think of it as the size of the invading army. The larger the army, the lower your odds at surviving. It begins with exposure. If you have on a mask and inhale a few virus cells, that is still not great, but it is a hell of a lot better than leaning over Uncle Bob as he coughs thousands of virus cells into your face where they are inhaled, go up nose, and into eyes infecting you with massive exposure. In scenario one, the few virus cells start multiplying, at the same time that your body starts identifying an antibody to start creating in order to fight back (i.e. building its protective army). By the time your defense army of antbodies is ready, the invading virus army is still small enough to effectively fight. In scenario #2 with Uncle Bob, you started with a much bigger invading army, and it reproduced exponentially faster. By the time your defensive antibody army is prepared – the invading virus army is already a great big monster, and you now have a much harder fight on your hands. Having good health, and a healthy probiotic system increases your bodies ability to more quickly create its own army, and at the same time slows down the invading virus army. So reducing viral load at all stages of the game is critical. And this is why you SHOULD wear a mask if you have one. I understand that the CDC wants the doctors and healthcare workers to have the protection, but it is very dishonest how they are trying to shame Citizens into not protecting themselves. NO, the masks are not a 100% protection, as referenced early in this article, but they can substantially reduce your initial viral load, and that literally can mean the difference between life and death. It is not your fault that the Government and Healthcare system wasn’t prepared. If you have masks – wear them. There is no dishonor in protecting yourself and your family, and the only shame is in those that tell you so.
Well, I could probably go on longer, but I believe that in my 20 years of preparing for and researching this – I have touched on several of the most important points that I feel are not being communicated as clearly as they should be. If anyone feels there is a substantial item/fact missing that needs clearer communication or discussion, please email the details to themtnsvoice@aol.com.
Good luck. This is just the beginning.
Peace,
– david / publisher
Focus on Big Canoe, GA
* a publication of The Mountains Voice
Media and Public Official Note: I do think Public Health Authorities and Health Media are recently doing a better than usual job of communicating, but they need to switch from focusing on the spread of the virus, and concentrate on educating the public on what they can do at all stages of the Outbreak. Obviously all needs to be done to slow the spread – but to pretend that this is containable at this point is to be willfully ignorant, or outright lying. I continue to suggest that people take things coming out of the CDC, WHO, and other National Health Departments with a grain of salt. Do your own research and take responsibility for your own preparation. It’s your life, your health.
On a Personal Reporting Note: I really don’t care what the spread situation is today, how many cases are in the U.S., etc. It doesn’t matter anymore. The only relevant fact regarding spread I am concerned with, is that it IS going to continue, and eventually it will be Local to me, no matter where in the world I go, and I need to plan accordingly and be prepared, and realize that a lot of things are going to change. The Global Health System is going to be decimated by this Global Outbreak, and people need factual Information that is going to be relevant to THEIR lives, especially given that there is No Vaccine coming to the rescue. When local and regional Healthcare Systems start collapsing from the sheer numbers of sick and dying (including healthcare workers) people will need to be able to treat themselves. One of my goals is to influence the Media to start looking at this through the lens of something that is completely new, and that the modern world has never seen before, and to consider the full spectrum of possibilities and facts in their reporting. It is the Media’s job to prepare and educate the people on ALL aspects of the developing situation.
Lastly on an Economic Note: SARS did $50 Billion in Economic damage and this is going to be hundreds of times worse. It is going to shut down most of global travel and tourism. It is going to slow business across the globe in almost every sector. It is going to take an already precarious global economic situation and push it over the edge. On a very, very short term good news point – I can hear those money-printing presses firing up for “Q.E. 4 to Infinity” already 🙂 Update February 4, 2020: China has fired up the printing presses to the tune of 700+ Billion. The Federal Reserve is now sending signals it might start QE4. With more and more bad economic nad pandemic news breaking – Stocks are back on track with the news of more free money printing, and are shooting for the moon as artificial stimuus rolls out it’s TEMPORARY fix. Beware the Pump-n-Dump!
Disclaimer: None of this is medical advice. Do your own research. Make informed decisions.
Some References:
There is a lot of talk about “fake news” regarding this WUHAN-CoV coronavirus outbreak. Unfortunately, much of it is coming from mainstream media, including our health officials. Just one example of irresponsible journalism is this Story from CNBC, misrepresenting the World Health Organization’s actual statement, which itself was a manipulation of Fact vs Myth. The WHO Statement says, “there is no evidence from the current outbreak that eating garlic has protected people from the new coronavirus.” Of course not, as this is a brand new virus and there has been no time to do any studies to get that “evidence”. HOWEVER, there is an enormous amount of data that shows that Garlic and it’s components (mainly Allicin and Joene) ARE effective against Viruses. In one 1973 Japanese Study, the conclusion was, and I QUOTE:
The experiment revealed that the garlic extract, contrary to Japanese encephalitis case, further heightened the preventive effect of influenza vaccines, and in the case of using alone it was as effective as vaccines.
So while the WHO is techincally not lying when they reference “no evidence from the current outbreak”, they are manipulating the facts, and effectively “lying by ommission” when they fail to reference the multitude of studies that do exist. And of course, the way the mainstream media story spun it WAS Outright Lying and Misepresentation. There are plenty of scientific studies backing p all the data I reference. Some is below. Please note that I am an article writer, and I am already providing more reference material that any mainstream media outlet, and even any health organization. I encourage people to do their own research. Email me <themtnsvoice@aol.com> with additional studies for consideration / reference as well.
Garlic Studies Summary: Garlic contains Allicin which is the main active component, though others exist. It is shown to have a multitude of benefits and anti-microbial and antiviral properties. It can also regulate cytokine activity and could be of benefit in fighting Cytokine Storm. Below is a partial sampling of studies.
Ref 1 / Ref 2 / Ref 3 / Ref 4 / Ref 5 / Ref 6 / Ref 7 / Ref 8 / Ref 9 /
licorice (aka glycyrrhizin; See Ref 1 / Ref 2 / Ref 3 )
Note: One side effect is that licirice and its compounds can lower Potassium levels. Might want to consider Potassium supplementation if using Licorice, and then usage only for the short duration of illness. My personal thoughts (not medical advice) is that I would only use licorice as a temporary
And for the record, neither Garlic nor Licorice is on my Shortlist of “Must Have” treatments, although I will also use them because they can’t hurt, and most lkely will help in some limited fashion. My point is not to push Garlic…. it is to push Truth, and the amount of misinformation and false narrative being pushed by the Media and Health officials is getting out of hand.
{kind=link}
Be the first to comment